Oncologist are cancer specialist. GI Oncologist deals with GI Cancers. Incidence of Gastrointestinal cancer has increased in the recent past. Upper GI Cancer include cancer of the esophagus, stomach, duodenum and small intestine. Cancer of the colon and rectum are lower GI cancer. Hepato-Biliary GI Cancer include cancer of the liver, gallbladder, bile duct and pancreas.
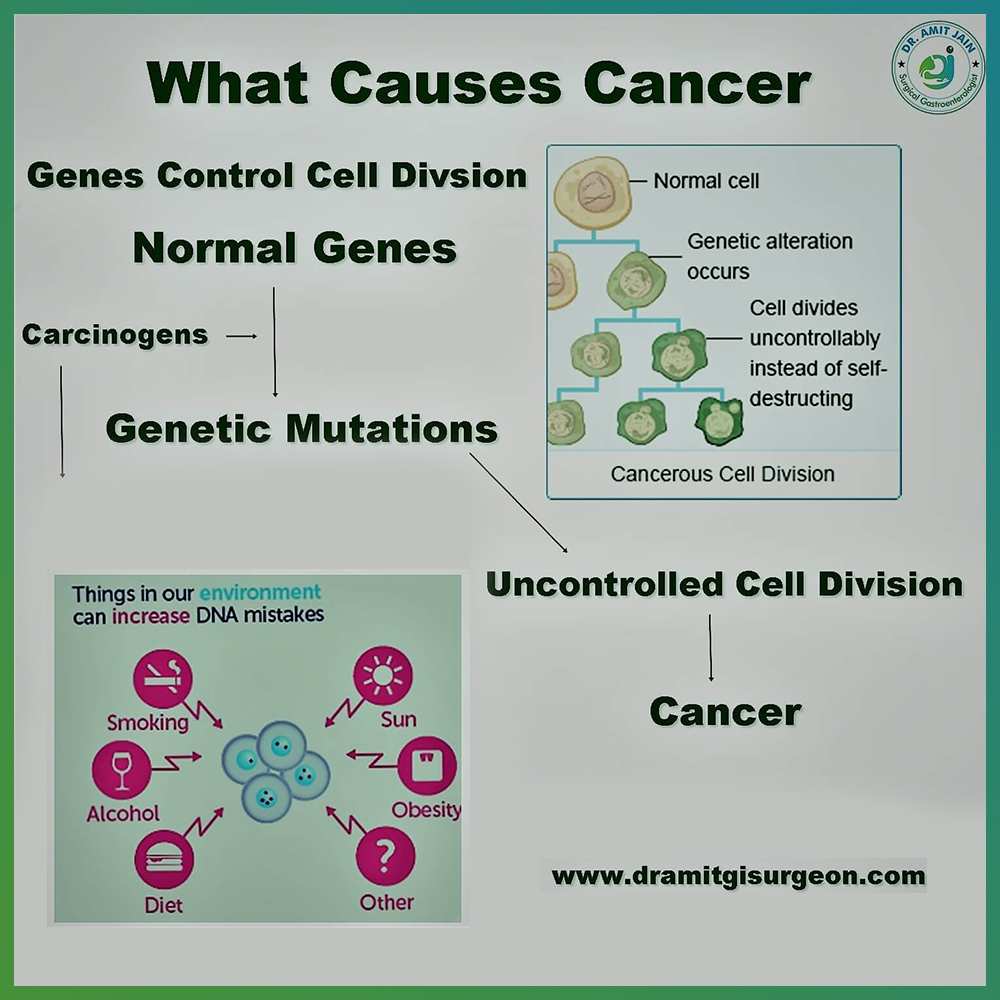
Cancer is uncontrolled cell division. Cells divide to replace old or dead cells. This process takes place in a controlled pathway so that the cells divide in required number only. This pathway is under gene regulation, cancer is caused by damage to these growth regulatory genes.
Damage to genes is caused by exposure to cancer causing substances called as carcinogens. It may be a chemical substance, such as certain molecules in tobacco smoke, environmental agents or viral
Uncontrolled cell division leads to formation of a mass of cancer cells. These cancer cells can dismantle from main or original mass of cells and through lymphatic system or blood can migrate or travel to other organs where again they can proliferate and form a mass of cancer cells. This whole process is termed as metastatic spread or metastasis when cancer cells leaves an area of origin and grow in another body part
Metastatic cancer are stage IV disease and carry a very bad prognosis.
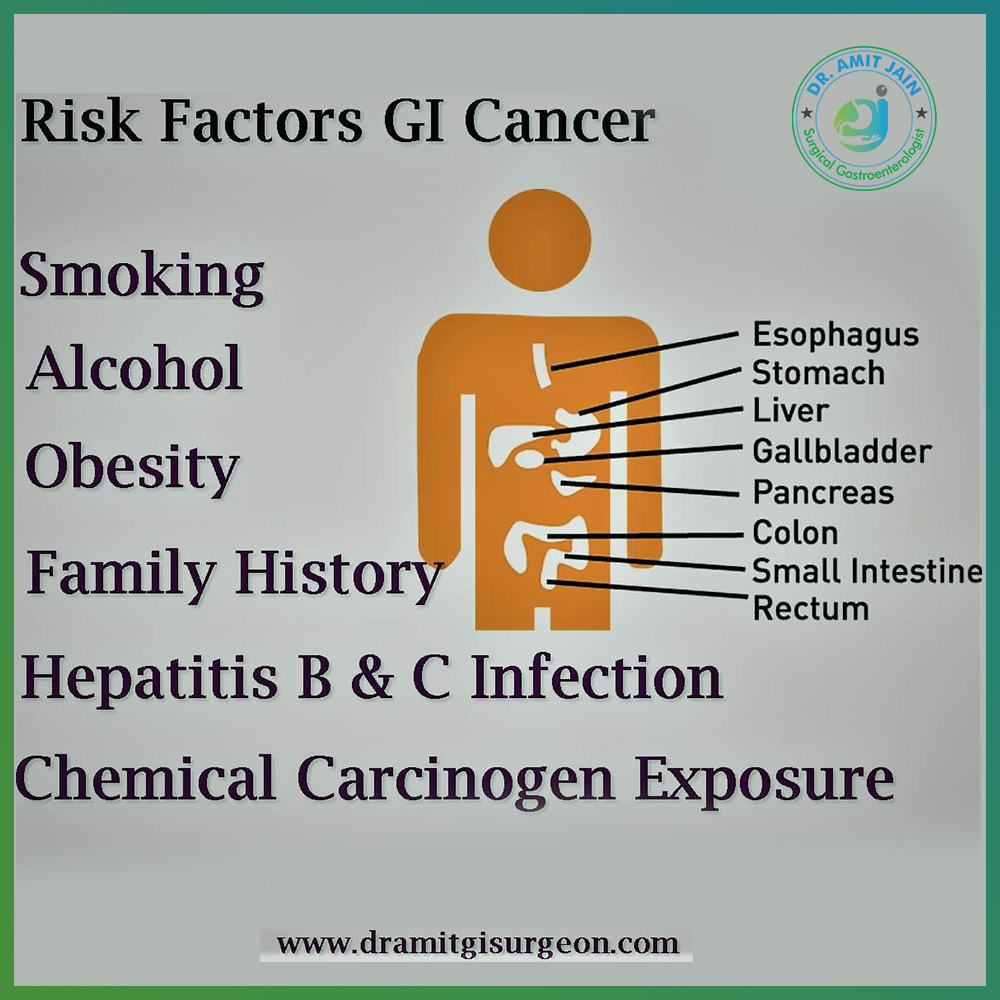
Cancer Risk Factors
Cancer risk factors can be divided into the following groups:
Biological factors which are non-modifiable such as age, gender, inherited genetic defects
Environmental exposure to radon and UV radiation
Occupational risk factors, include exposure to many chemicals, radioactive materials and asbestos
Lifestyle-related factors which include alcohol, smoking, obesity. These are the most common and easily preventable cause of GI Cancer
Viral Infections: Hepatitis B & C. Hepatitis B vaccine is available and Hepatitis C is treatable. Inspite of this more than 50% the cause of liver cancer is these viral infections
Follow Oncologist Advise & Reduce Your Cancer Risk
Don’t use tobacco: Smoking & Chewing tobacco has been linked to various types of cancer . Avoiding tobacco or deciding to stop using it is an important part of cancer prevention.
Eat a healthy diet: Eat plenty of fruits and vegetables. Base your diet on fruits, vegetables and other foods from plant sources such as whole grains and beans.
Maintain a healthy weight and be physically active. Obesity is a risk factor for esophageal and liver cancer. Overweight causes fatty liver which is an important cause of hepatic cancer. This is the reason many a times oncologist stress on maintaining healthy weight to prevent from these deadly cancers
Get Vaccinated against Hepatitis B infection.
Avoid alcohol intake.


Symptoms of Gastrointestinal Cancer
Vomiting: It occurs when there is an obstruction in the gastrointestinal tract. Obstruction distal to the bile duct opening causes billious vomiting. Obstruction proximal to it causes non-billious vomiting. Primary stomach cancer or small bowel cancer causes vomiting due to intrinsic mass which compromise the lumen. Gallbladder Cancer can cause external compression over the duodenum and antro-pyloric region resulting in gastric outlet obstruction
Jaundice: It occur when there is obstruction in the Common bile duct. This obstruction can be intrinsic due to bile duct cancer. It may be extrinsic due to external compression such as Gallbladder mass or pancreatic head mass causing external compression over the CBD. Patient present with features of surgical obstructive jaundice such as pale colored stool, dark urine and pruritus
Dysphagia: Early and common symptom of esophageal cancer. Patient has initially dysphagia to solid foods and gradually progress to liquid. This progressive dysphagia is indicative of any progressive mass lesion which is compromising the esophagus lumen and causing dysphagia
Melena: It is passage of black tarrish colored stool. Melena indicate slow bleed in the GI tract. This bleed can originate at any site along the GI tract. Cancer stomach and peri-ampullary cancer and right sided colon cancer have a tendency to bleed. Sometimes patient have occult bleed and present with feature of anemia such as weakness/tiredness
Hematochezia: It is the passage of fresh blood per rectum. Small amount of fresh blood with stool indicate cancer rectum
Anorexia and Weight Loss: these are common symptoms of any malignancy in our body
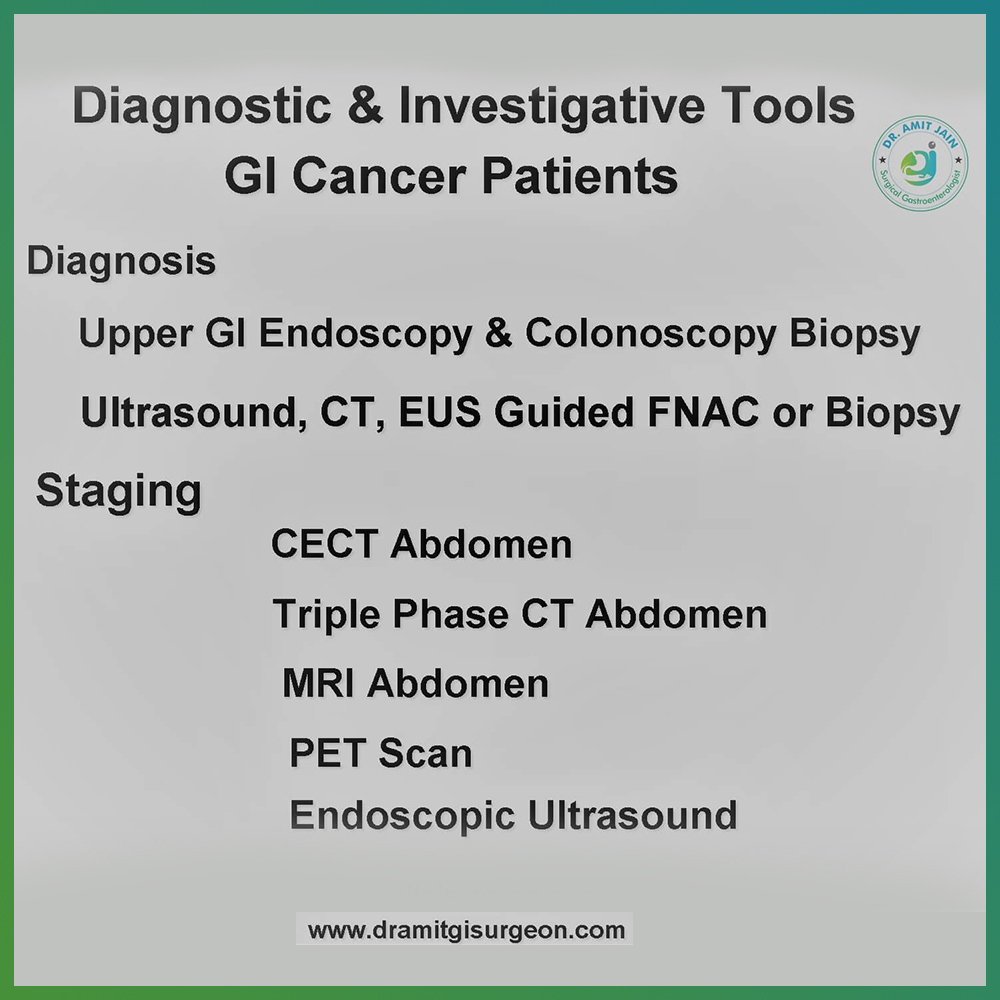
Diagnosis & Staging
The purpose of investigations in patients presenting with symptoms & signs s/o GI cancer is to establish or confirm the diagnosis and to further stage the tumor
Diagnostic Tools
Upper GI Endoscopy is done for symptoms s/o esophagus, stomach and duodenal cancer. Growth can be visualized and biopsy can be taken
Colonoscopy for suspected Colo-Rectal Cancer. In patients with rectal cancer, full length colonoscopy should be done as the incidence of synchronous malignancy is high in these patients
FNAC (Fine Needle Aspiration Cytology): For solid organs such as Liver, pancreas and gallbladder FNAC can be done to establish the diagnosis. However there is risk of seedling the cancer cells in the needle track, thats why it should be avoided. Only when pre-operative chemotherapy or radiotherapy is needed, it is done to confirm the diagnosis
Staging Tools
CT Scan: CECT chest and upper abdomen for esophageal cancer. Triple Phase CT abdomen for Liver, Gallbladder and Pancreas Cancer.CECT whole abdomen for stomach, small intestine and colorectal cancer
PET-Scan: The sensitivity of PET scan to diagnose metastases missed on CT scan is more, however there is high false positive rate also, so it is done selectively in high risk patients and large bulky tumors
EUS (Endoscopic Ultrasound): It is advance diagnostic & staging tool in the management of GI cancer patients. At the tip of endoscope a ultrasound probe is placed and inserted like an upper GI endoscope
Definitive Treatment
GallBladder: Radical cholecystectomy in which gallbladder is removed along with liver wedge and lymphadenectomy is done if the tumor is resectable. Cystic duct margin is sent for biopsy intra-op. If biopsy comes to be positive then Common Bile duct excision along with Roux-en-Y Hepaticojejunostomy is done
Liver: Options are Liver resection, Transplant, local ablative procedures such as Radio frequency ablation (RFA) & Trans-arterial embolization (TACE)
Local ablative procedure such as RFA is curative up to lesion of size 2cm; Other such as TACE is non-curative. Theses procedures are used as a bridge to liver transplant or to downstage tumor before transplant
A Multi modality approach is required for the management of HCC. It is a team work involving Hepato-biliary surgeon, Oncologist and Hepatologist. Best hospital for liver cancer treatment are tertiary care level hospitals where all infrastructures and specialist doctors are available under one roof
Pancreas: The standard surgical procedure done in case of tumor located in head of pancreas is whipple procedure (pancreatico-duodenectomy). If it is located in the distal part distal pancreatectomy with splenectomy is done. Patient with a head tumor can have jaundice. Pre-operative biliary stenting is done if the bilirubin level is very high, patient has fever and poor general condition with poor nutrition. Most of the medical oncologist advice pre-operative chemotherapy in locally advance pancreatic cancer
Esophagus: Radical Esophagectomy is done in which esophagus is removed and a stomach tube is created which is anastomosed to esophagus in the neck.
Stomach: Radical gastrectomy is done. Depending on the location of tumor radical distal gastrectomy or radical sub-total gastrectomy or radical total gastrectomy is done. At least 12 lymph nodes should be dissected in the resected specimen for completeness of lymphadenectomy
Colo-Rectal: The standard surgical treatment of colon cancer is radical colectomy. Colon is divided into four parts, ascending or right colon, transverse colon, descending or left colon and sigmoid colon. Depending on location of cancer respective colectomy is done. After colonic resection depending on patient nutrition status and tumor burden either anastomosis is done or stoma is created. For Rectal cancer Anterior Resection is done. For Locally advanced rectal cancer pre-operative chemo-radiotherapy is given medical oncologist, which has shown to increase the survival rate
Laparoscopic GI Cancer Surgery
Laparoscopic surgery was initially done for benign gastrointestinal diseases. With advance in technology and instrumentation it was further extended for cancer surgery also. Now there is lot of data in literature which suggest that laparoscopic surgery in cancer patients is safe as open surgery. Long term survival rate in cancer patients in laparoscopic surgery is also same as open surgery.
GI Cancer surgeon who have special training in Laparoscopic surgery do such surgery laparoscopic. With advancement in instrumentation & energy source device this approach has become safe and more convenient to surgeons also
For Luminal cancer such as esophagus, stomach and Colo-rectal, this approach has been used since long time. Colon & Rectal cancer are the two most common GI malignancy which are routinely done by minimally invasive approach.
For solid GI malignancy such as Liver, gallbladder & pancreas, high volume centers are doing it routinely and with same results as compared to open approach

Palliative Treatment For Stage IV or Metastatic Disease
Surgery is the treatment of choice in gastrointestinal cancers if the tumor is resectable and patient is fit for surgery. Gastroenterologist play an important role if the tumor is advanced and metastatic, as most of these symptoms can be palliated endoscopically.
Dysphagia is the most common symptom of esophagus cancer and the best way of palliation is endoscopic placement of esophagus stent across the site of obstruction. In similar way in patients of stomach cancer and duodenal cancer who have gastric outlet obstruction and have vomiting, stent can be placed across the obstruction site and vomiting can be relieved. Patients of esophagus and stomach cancer can present with hematemesis or melena. It indicate tumor site bleed. Many a times these bleeds can be controlled endoscopically
Growth in the colon or rectum can cause bowel obstruction. Many a times these patients present in emergency with features of large bowel obstruction such as abdomen distension, vomiting, not passage of flatus and motion. When investigated further are found to have advanced colo-rectal cancer. In these patients endoscopically stent can be placed and obstruction can be relieved. A major surgery can be avoided in these patients
Most common hepato-biliary cancer symptom which require palliation is jaundice. Jaundice is either due to primary cancer such as cholangiocarcinoma or it may be caused by external compression by nearby organ malignancy. Gallbladder neck mass, periampullary cancer, pancreatic head mass malignancy are common GI Cancer which can cause jaundice.Endoscopic internal biliary stenting is best palliation for these patients
GI Cancer Management: Team Work Involving Specialized Oncosurgeon, Gastroenterologist, Medical & Radiation Oncologist & Intervention Radiologist
Surgical Gastroenterologist are GI Cancer Surgeons or GI Oncosurgeons are trained in the field of GI Surgery. They have vast experience in surgical management of these patients
Medical Gastroenterologist have role from diagnosis to palliative care of these patients. Upper GI Endoscopy or Colonoscopy make the diagnosis. Endoscopic placement of stent in the esophagus, CBD and rectum provide symptomatic relief in advance cancer
Medical Oncologist are specialized physicians for medical management of cancer who give chemotherapy. It may be given in the pre-operative period in locally advance tumors to make it resectable. After surgery to increase the survival rate or in metastatic disease as palliation. There are some tumors which respond to radiation. In these cancers, Radiation Oncologist is involved to provide his expertise
Neo-Adjuvant Therapy
Surgery is the treatment of choice for most of the gastrointestinal cancer. However for locally advanced tumor ( Tumor with T2 stage or beyond and lymph node positive) literature support chemotherapy or radiotherapy or both in combination before surgery, which has shown to improve survival rate. This treatment before surgery is called as neo-adjuvant therapy
Gastrointestinal Cancer At Young Age ? What Oncologist Says
The incidence of gastrointestinal cancer is increasing; Generally cancer is disease of old age but nowadays it is being frequently seen in young population also, mostly gallbladder and colo-rectal cancer.Studies show incidence is increasing because of our life style and dietary habits
Adult obesity is the main cause of increased Colo-rectal cancer seen in this age group. The main symptom is lower GI bleed. Any young patient with such symptom should be evaluated completely and colonoscopy must be advised to rule out Colo-rectal cancer
Most cancer detected in this age group are advanced or metastatic. It may be due to either tumor biology which may be more aggressive in young age or it may be cancer is not suspected in these patients because of young age and diagnosed at later stage
Anorexia & weight loss are two common consistent symptom and sign of any cancer and when patient of any age group present with same should be thoroughly investigated to rule out any malignancy

World Abdominal Cancer Day
The aim is to raise awareness about cancer prevention, detection & treatment. It is an international event celebrated on 19th May every year.The primary goal is to reduce morbidity and mortality due to cancer.
Cancer Screening
Cancer starts in our body, before we develop any symptoms. Cancer Screening is a method to detect cancer at this stage when we do not have any symptoms. Normal risk people are not candidates for screening. It is only applicable for high risk individuals such as chronic liver disease patients who are prone to have hepatic cancer and ulcerative colitis patients to develop colorectal cancer
Early diagnosis & treatment is key to increase the survival rate in cancer patients. If we can detect tumor in these high risk patients at early stage and treat, chances of success is very high
Most Oncologist agree that another major role of screening is prevention of cancer. It has been known that colo-rectal cancer develops from pre-cancerous lesions called as polyps. The chances to harbor these lesions is more after the age of 50 year. It has been recommended that at the age of 50 year, colonoscopy should be done in all normal risk individuals to detect these polyps and should be excised before these convert into cancer. Remember prevention is always better than cure